

April 2, 2021 | By J. Paul Spencer, CPC, COC
We now collectively find ourselves one calendar quarter into the new frontier of 2021 outpatient E/M services.
Since January 1, I have fielded many questions from my professional contacts regarding how best to look at the newly-engineered medical decision making (MDM) component. As might have been expected, some gray areas presented themselves as clinics across the country implemented the new standards. This led to the AMA putting forward technical corrections on March 9 that addressed areas requiring clarification. In response to this document, NAMAS held a panel webinar on these revisions, which was recorded and can be replayed here.
While revisions are usually expected when such a big change comes forward, suddenly we are confronted with a completely different set of “technical corrections.”
P.T. Barnum once said that nobody ever lost a dollar by underestimating the taste of the American public. To paraphrase Mr. Barnum in a similar vein, no one in our industry ever looked foolish elucidating the vexing nature of a typical insurance denial, and for today’s Tip of the Week in the year A.D. 2021, we have a doozy, shared with us by Stephanie Allard:
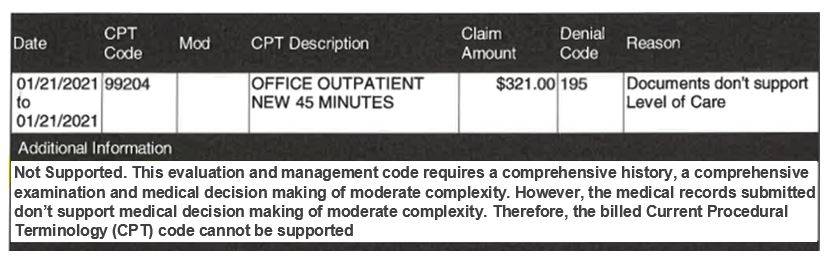 As we can see from this denial, this is a 2021 date of service billed using outpatient new patient E/M code 99204. What is curious is that the denial reason uses language geared towards pre-2021 E/M services, indicating that this E/M code “requires” a comprehensive history and examination. Mentioning the history and examination “components” under the current paradigm, in any way other than to state that the documentation of either is “medically appropriate,” is not an accurate statement, and should not be appearing on explanations of benefits for 2021 services.
As we can see from this denial, this is a 2021 date of service billed using outpatient new patient E/M code 99204. What is curious is that the denial reason uses language geared towards pre-2021 E/M services, indicating that this E/M code “requires” a comprehensive history and examination. Mentioning the history and examination “components” under the current paradigm, in any way other than to state that the documentation of either is “medically appropriate,” is not an accurate statement, and should not be appearing on explanations of benefits for 2021 services.
Yet that is only one aspect of the problem with this particular denial. We also have a statement that indicates that a review of the medical records for this service didn’t support medical decision making of moderate complexity. Since this portion of the denial does apply to 2021 E/M guidelines, we decided to take a look at the documentation for this service.
In this encounter, a new patient to the practice with a complicated presentation, including a history of another disease process, was evaluated and managed. The provider planned additional workup in order to better define and diagnose the patient’s condition, as well as to assess the damage that the patient had suffered previously due to inflammation. Six separate lab tests were ordered, and the physician had a lengthy discussion with the patient regarding drug use for chronic pain management. It is important to point out that in this specific case, there was no documentation of the total time of the encounter.
Based on documentation of a presenting problem that is new to the examining physician, that is undiagnosed and with an uncertain prognosis, requiring additional workup, coupled with the complexity of this problem, and prescription drug management, the MDM for this visit most certainly supports a moderate level of complexity based on 2021 guidelines.
I have always believed that appeals of determinations by an insurance carrier or contractor is first and foremost about establishing precedent. The most important thing you can do, particularly as it applies to 2021 and beyond for office/outpatient E/M services, is to put payers on notice that erroneous denials such as this will not be tolerated. The easiest way to do this is by appeal. Given the low risk/reward of an individual appeal, it may be more cost-effective to bundle similar denials into one appeal, or to submit multiple single, similar denials all at once to reduce the costs of appeals.
Understand that a large portion of this denial could simply be a case of an insurer not adequately modifying automated language for denial reasons that are placed on EOBs. Nevertheless, in the meantime, it provides opportunities to appeal based on erroneous information, which should (stress on the word “should”) create a level of embarrassment for the carrier.





