

January 15, 2021 | By Stephanie Allard, CPC, CEMA, RHIT
CMS defines critical care as “the direct delivery by a physician(s) of medical care for a critically ill or injured patient. The care of such patients involves decision making of high complexity to assess, manipulate, and support central nervous system failure, circulatory failure, shock-like conditions, renal, hepatic, metabolic, or respiratory failure, postoperative complications, overwhelming infection, or other vital system functions to treat single or multiple vital organ system failure or to prevent further deterioration. It may require extensive interpretation of multiple databases and the application of advanced technology to manage the patient. Critical care may be provided on multiple days, even if no changes are made in the treatment rendered to the patient, provided that the patient’s condition continues to require the level of physician attention described above.”
“Critical care services include but are not limited to, the treatment or prevention or further deterioration of central nervous system failure, circulatory failure, shock-like conditions, renal, hepatic, metabolic or respiratory failure, postoperative complications, or overwhelming infection. Critical care is usually, but not always, given in a critical care area, such as the coronary care unit, intensive care unit, pediatric intensive care unit, respiratory care unit, or the emergency care facility.”
There are two important takeaways from this definition. First, critical illness or injury is something that acutely impairs one or more vital organ systems such that there is high probability of imminent and life-threatening deterioration in the patient’s condition.
Second, that critical care involves high complexity decision making to assess, manipulate and support vital system function(s) to treat single or multiple vital organ system failure and/or to prevent further life-threatening deterioration of the patient’s condition.
Critical Care Documentation
Based on the detailed definition we have, the following elements of documentation should be included to support billing of the critical care code(s):
- Organ system failure
- Immediate action required to support life
- What services were provided to the patient that met the definition of critical care impacting an episode of care
- Total time of the critical episode, details below:
- Total duration of time spent in provision of critical care services to a critically defined patient
- Time does NOT have to be continuous, provided the time counted required the provider’s devoted attention
- Includes time at patient’s bedside or elsewhere on the floor or unit
- Includes discussion with family members when patient is compromised
- The patient is unable or incompetent to participate in giving history and/or making treatment decisions
- The necessity to have the discussion (e.g., “no other source was available to obtain a history” or “because the patient was deteriorating so rapidly, I needed to immediately discuss treatment options with the family”)
- Medically necessary treatment decisions for which the discussion was needed
- A summary in the medical record that supports the medical necessity of the discussion
- All other family discussions, no matter how lengthy, may not be additionally counted towards critical care. Telephone calls to family members and or surrogate decision-makers may be counted towards critical care time, but only if they meet the same criteria as described in the aforementioned paragraph
- If any time was spent working with ANY other patient during this time, critical care would not be supported
- Provide specific wording to indicate “critical care”
Critical Care Statement
Critical care cannot be billed on the macro statement and documentation of critical care time alone. It is important to read the entire note to ensure that overall the documentation shows the patient’s critical status and need for life-saving management. Critical care cannot be assumed based on a critical care time statement, the patient’s diagnoses and/or location/unit floor (i.e., just because a service is rendered in the ICU or another critical unit does not automatically make it a critical care service). If the documentation of the history, exam and medical decision making contradicts the critical care statement, critical care should not be coded.
Example: If the below critical care statement is included in a note, but the documentation shows patient improvement and stabilization following de-escalation of care, critical care would not be supported even with this statement.
This patient has a high probability of sudden clinically significant deterioration which requires the highest level of physician preparedness to intervene urgently. I managed/supervised life or organ supporting interventions that required frequent physician assessments. I devoted my full attention in the ICU to the direct care of this patient for this period of time. Organ systems which are failing and require intensive critical care support are: Neurological, hydrocephalus.
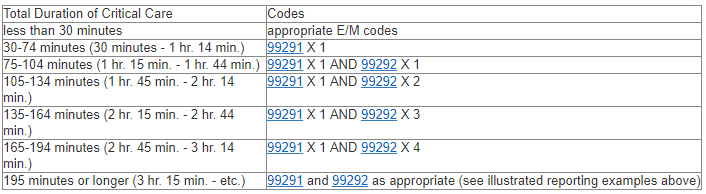
Critical Care Time Thresholds
Critical Care Bundled Services
Time involved performing procedures that are not bundled into critical care (i.e., billed and paid separately) may not be included and counted toward critical care time. The physician’s progress note(s) in the medical record should document that time involved in the performance of separately billable procedures was not counted toward critical care time.
The following services are included in the critical care code(s) when performed during the critical period by the physician(s) providing critical care:
- The interpretation of cardiac output measurements (93561, 93562), chest X-rays (71045, 71046), pulse oximetry (94760, 94761, 94762), blood gases
- Collection and interpretation of physiologic data (e.g., ECGs, blood pressures, hematologic data)
- Gastric intubation (43752, 43753)
- Temporary transcutaneous pacing (92953)
- Ventilatory management (94002-94004, 94660, 94662)
- Vascular access procedures (36000, 36410, 36415, 36591, 36600)
- Any services performed that are not included in this listing should be reported separately
Critical Care Provided by Multiple Providers of the Same Specialty
A split/shared E/M service performed by a physician and a qualified NPP of the same group practice (or employed by the same employer) cannot be reported as a critical care service. Critical care services are reflective of the care and management of a critically ill or critically injured patient by an individual physician or qualified non-physician practitioner for the specified reportable period of time.
Unlike other E/M services which can be split/shared if the requirements are met, critical care services reflect the evaluation, treatment and management of a patient by an individual provider and therefore cannot be reported for a combined service between a physician and a qualified NPP.
- Separate the type of provider involved
- NPP, MD, and DO
- We cannot combine time across provider types
- The first provider to see the patient on the DOS will bill 99291 and if time supports 99292
- The second provider to see the patient on the DOS can only bill 99292
- When CPT code time requirements for both 99291 and 99292 and critical care criteria are met for a medically necessary visit by a qualified NPP the service shall be billed using the appropriate individual NPI number. Medically necessary visit(s) that do not meet these requirements shall be reported as subsequent hospital care services.
- Report the appropriate code(s) for the total time spent per provider type
- First provider – 99291 and 99292
- Second provider – 99292
Critical Care With Resident Involvement
Time spent teaching may not be counted towards critical care time. Nor can the teaching physician count time spent solely by the resident (in the teaching physician’s absence) toward critical care or other time-based services. Only time that the teaching physician spends alone with the patient (and that he/she and the resident spend together with the patient), can be counted toward critical care time.
A combination of the teaching physician’s documentation and the resident’s documentation may support critical care services. Provided that all requirements for critical care services are met, the teaching physician documentation may tie into the resident’s documentation. The teaching physician may refer to the resident’s documentation for specific patient history, physical exam findings and medical assessment.
However, the teaching physician’s medical record documentation must provide substantive information including:
- Time the teaching physician spent providing critical care
- That the patient was critically ill during the time the teaching physician saw the patient
- What made the patient critically ill
- The nature of the treatment and management provided by the teaching physician.
If the teaching physician did not see the patient together with the resident, it is important for the teaching physician’s documentation to support the critical care services without relying on the resident’s documentation. In this scenario, the resident’s documentation would support the work that they performed independently which cannot be combined with the teaching physician to bill for critical care services. If the teaching physician’s documentation does not support critical care services the initial or subsequent E/M code would have to be billed in place of critical care. If an initial or subsequent E/M is billed, you can combine the resident’s note along with the teaching physician to support 99221-99223 or 99231-99233.





